When your lungs start to stiffen and lose their ability to expand, breathing becomes a struggle-not just during exercise, but even at rest. This isn't just aging. It could be interstitial lung disease (ILD), a group of more than 200 conditions that cause progressive scarring deep within the lung tissue. Unlike infections or asthma, ILD doesn’t go away with rest or medication. The damage is permanent. But early detection and the right treatments can slow it down-and help you keep living well for as long as possible.
What Exactly Is Interstitial Lung Disease?
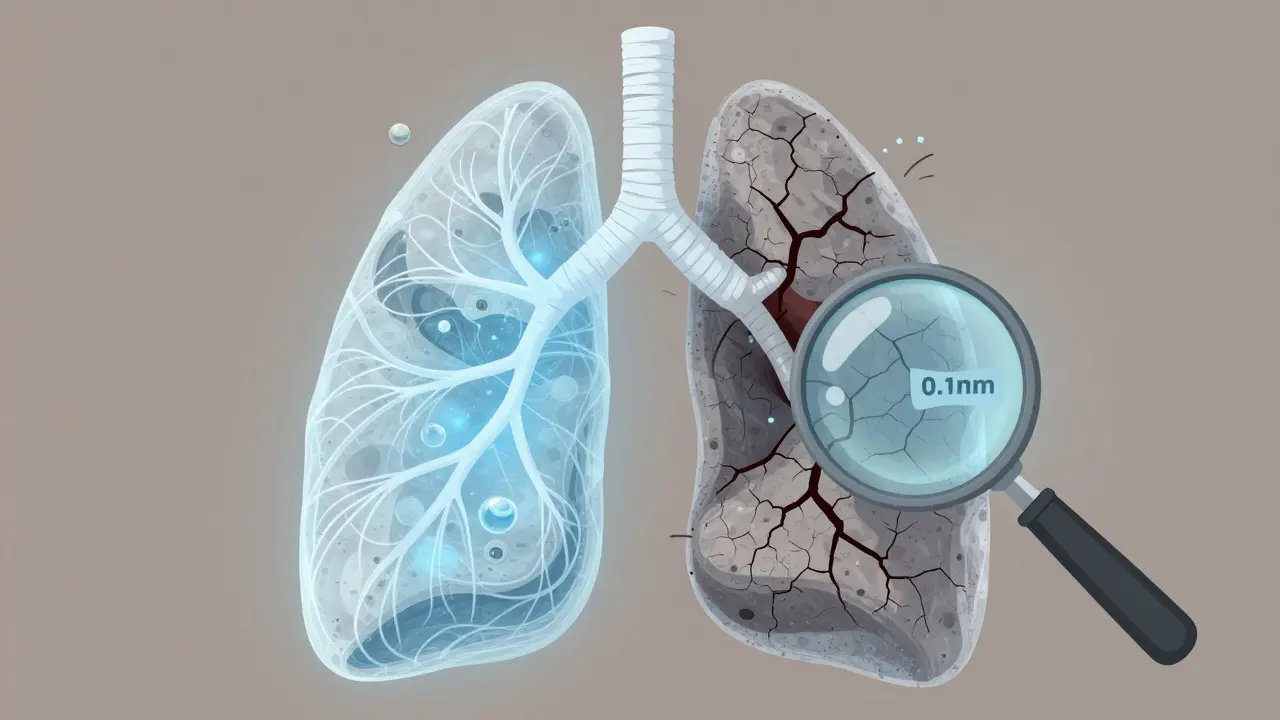
ILD affects the interstitium, the thin layer of tissue between the air sacs (alveoli) in your lungs. Think of it like the scaffolding that holds the air sacs in place. In healthy lungs, this tissue is less than 0.1mm thick. In advanced ILD, it thickens to 1-2mm or more, turning flexible, stretchy lung tissue into stiff, fibrous scar tissue. This makes it harder for oxygen to pass into your bloodstream and for carbon dioxide to leave.
It’s not one disease. It’s a category. The most common form is idiopathic pulmonary fibrosis (IPF), which makes up 20-30% of all ILD cases. IPF has no known cause, which is why it’s called “idiopathic.” Other types come from autoimmune diseases like rheumatoid arthritis or lupus, long-term exposure to dust or chemicals (like asbestos or silica), radiation therapy, or even some medications. In about 15% of cases, it’s sarcoidosis-a condition where clusters of inflammatory cells form in the lungs and other organs.
What all these forms have in common is progressive scarring. Once the lung tissue is scarred, it can’t heal. That’s why catching ILD early is so critical. By the time symptoms become obvious, damage is already done.
How Do You Know You Have It?
ILD doesn’t hit you with a sudden cough or fever. It creeps in. Most people first notice shortness of breath during activity-climbing stairs, walking uphill, carrying groceries. At first, they blame it on being out of shape. Then the breathlessness gets worse. It starts happening even when sitting still. A dry, hacking cough follows, often without mucus. Fatigue becomes constant. Some people notice their fingertips thickening or curving at the tips-a sign called clubbing, seen in 35-50% of IPF cases.
According to UCHealth’s 2023 clinical data, 92% of ILD patients report dyspnea. Nearly 80% have a persistent dry cough. About 65% feel exhausted all the time. In advanced cases, oxygen levels in the blood drop below 88%, forcing patients to use supplemental oxygen at rest.
Pulmonary function tests show clear patterns: forced vital capacity (FVC) drops by 20-50%, and the diffusing capacity for carbon monoxide (DLCO) falls by 30-60%. These numbers don’t lie. They tell doctors how much lung function is lost.
But here’s the catch: many patients go undiagnosed for years. A 2023 survey from Pulmonary Fibrosis News Forums found that 78% of patients had been misdiagnosed at least once-often as asthma, COPD, or just “getting older.” The average time from first symptom to correct diagnosis? Over 11 months.
What Does the Damage Look Like?
High-resolution CT scans (HRCT) are the gold standard for diagnosing ILD. These scans show the scar tissue in fine detail-areas of honeycombing, reticulation, or ground-glass opacities. But even experts miss early signs. Dr. Athol Wells noted in 2022 that current imaging techniques fail to detect subtle fibrosis in 20% of early cases.
Progression varies wildly between types:
- IPF: FVC declines 200-300 mL per year. Median survival without treatment is 3-5 years.
- Rheumatoid arthritis-ILD: Slower progression. 70-80% survive at least 5 years.
- Sarcoidosis: 60-70% improve on their own within 2 years.
- Drug-induced ILD: Often reverses after stopping the medication.
- Acute interstitial pneumonitis: 60-70% die within 3 months, even with ICU care.
Environmental exposures like asbestos lead to slower decline (100-150 mL/year FVC loss), while idiopathic forms race ahead. That’s why knowing the cause matters as much as the symptoms.
Treatment: Slowing the Scarring
There’s no cure. But there are treatments that can slow the scarring and help you breathe better.
The two FDA-approved drugs for IPF are nintedanib (Ofev®) and pirfenidone (Esbriet®). Both are antifibrotics-meaning they target the process that creates scar tissue. In clinical trials, they cut the rate of FVC decline by about 50% over a year. That doesn’t mean you’ll get better. But it means you might not get worse as fast.
Side effects are real. About 65% of people on pirfenidone get sun-sensitive rashes. Nearly 60% report nausea, vomiting, or diarrhea. Nintedanib causes diarrhea in up to 70% of users. Dose adjustments are common. Still, many patients say the trade-off is worth it.
In September 2023, the FDA approved a third drug: zampilodib. It’s the first new antifibrotic in nearly a decade. In the ZENITH trial, it reduced FVC decline by 48% compared to placebo. It’s not yet widely available, but it’s a sign that progress is happening.
For non-IPF forms of ILD, these drugs often don’t help. That’s a major gap. As Dr. Talmadge King Jr. pointed out in 2021, “Antifibrotic medications show minimal benefit in non-IPF ILD subtypes.” That’s why research is shifting toward subtype-specific therapies.
Beyond Medication: Supportive Care
Medication alone isn’t enough. Pulmonary rehabilitation is one of the most effective tools you can use. These programs last 8-12 weeks and include supervised exercise, breathing techniques, nutrition counseling, and education. In UCHealth’s 2023 study, 72% of participants reported moderate to significant improvement in their ability to walk and do daily tasks. On average, they gained 45-60 meters in their 6-minute walk distance.
Oxygen therapy becomes necessary when resting blood oxygen falls below 88%. About 55% of IPF patients need it within two years of diagnosis. Proper oxygen equipment training is essential-mistakes can lead to dangerous drops in oxygen levels.
Energy conservation techniques help too. Simple changes-sitting while brushing your teeth, using a rolling cart for groceries, pacing activities-can make a big difference. Occupational therapy usually takes 4-6 weeks to teach these skills effectively.
And don’t ignore mental health. A 2022 American Lung Association survey found that 68% of ILD patients struggled with anxiety over breathlessness. Nearly half cut back on social activities because of oxygen tanks or fear of running out of air.

What’s on the Horizon?
The future of ILD care is moving fast. In October 2023, the American Thoracic Society added blood biomarker testing to its guidelines. Testing for the MUC5B gene mutation can now predict who’s likely to develop rapid IPF progression-with 85% accuracy.
Artificial intelligence is helping too. Mayo Clinic’s November 2023 study showed AI analyzing HRCT scans could identify ILD subtypes with 92% accuracy-better than human radiologists (78%). This means faster, more precise diagnoses.
Researchers are now studying over 14 genes linked to ILD susceptibility. The goal? Personalized treatment based on your genetic profile. Clinical trials are testing stem cell therapies, new tyrosine kinase inhibitors, and combination drug approaches. The global ILD drug market is expected to hit $3.42 billion by 2028.
But the biggest breakthrough might be early detection. The Pulmonary Fibrosis Foundation’s 2023 research agenda says screening high-risk groups-like smokers or people with autoimmune diseases-using blood biomarkers and targeted CT scans could cut diagnosis time by 40%.
What Should You Do If You Suspect ILD?
If you’re over 50, have unexplained shortness of breath, a dry cough, and fatigue that won’t go away:
- See a pulmonologist-not just your primary care doctor. ILD is often missed in general practice.
- Request a high-resolution CT scan of your chest. This is non-negotiable.
- Ask for a multidisciplinary evaluation. That means a pulmonologist, radiologist, and sometimes a pathologist reviewing your case together.
- Get pulmonary function tests done. Track your FVC and DLCO over time.
- If diagnosed, ask whether you’re a candidate for antifibrotic therapy.
- Enroll in pulmonary rehab. It’s not optional-it’s essential.
Don’t wait for symptoms to get worse. ILD doesn’t reverse. But it can be managed. The sooner you act, the more control you have over your life.
Is interstitial lung disease the same as pulmonary fibrosis?
No, but they’re closely related. Pulmonary fibrosis is a type of interstitial lung disease (ILD). ILD is the umbrella term for over 200 conditions that cause scarring in the lung tissue. Pulmonary fibrosis specifically refers to the scarring itself. Idiopathic pulmonary fibrosis (IPF) is the most common form of ILD, but not all ILD leads to fibrosis. Some types, like sarcoidosis, may cause inflammation without permanent scarring.
Can you live a normal life with interstitial lung disease?
It’s not possible to live exactly as you did before diagnosis, but many people live full, meaningful lives for years after diagnosis. The key is early intervention. With antifibrotic drugs, pulmonary rehab, oxygen therapy, and lifestyle adjustments, patients often maintain mobility, independence, and social engagement. A 2023 UCHealth study found that 72% of patients in rehab programs reported improved daily function. Quality of life depends heavily on how early treatment begins and how well complications are managed.
What triggers a sudden worsening of ILD?
An acute exacerbation is a sudden, unexplained drop in lung function. It can be triggered by infections (like pneumonia or the flu), heart failure, inhaling irritants, or even unknown causes. In IPF, about 10% of patients experience an acute exacerbation each year. These events are dangerous-up to 50% of patients don’t survive the first one. That’s why avoiding illness (getting flu and pneumonia vaccines), staying away from smoke or dust, and knowing the warning signs (worsening breathlessness, fever, new cough) is critical. Early hospitalization improves survival.
Are there any natural remedies or supplements that help ILD?
There’s no scientific evidence that vitamins, herbs, or supplements can slow lung scarring in ILD. Some people try N-acetylcysteine (NAC), antioxidants, or fish oil, but studies show no meaningful benefit in IPF. In fact, some supplements can interfere with medications. The only proven treatments are FDA-approved antifibrotics, pulmonary rehab, oxygen therapy, and lifestyle changes. Always talk to your pulmonologist before taking anything new-even something labeled “natural.”
How do you know if your ILD treatment is working?
Your doctor will track several things. The most important is your forced vital capacity (FVC) over time. A stable or slowly declining FVC (less than 100 mL per year) suggests the treatment is working. Your 6-minute walk distance is also monitored-improvement or stability is a good sign. Oxygen needs should stay steady or decrease. And most importantly, your symptoms: if you’re less short of breath, more energetic, and able to do daily tasks without fatigue, that’s a real-world sign of success. Regular follow-ups every 3-6 months are essential.
Is lung transplant the only option for advanced ILD?
Lung transplant is the only option that can replace damaged lung tissue, but it’s not for everyone. It’s reserved for patients with rapidly progressing disease who are otherwise healthy enough to survive surgery. Eligibility depends on age (usually under 70), absence of other serious illnesses, and strong social support. About 50% of transplant recipients survive at least 5 years. However, the waiting list is long, and not all ILD patients qualify. Many choose to focus on maximizing quality of life with existing treatments instead of pursuing transplant.
Comments (12)
Marissa Staples
March 25, 2026 AT 08:44It’s wild how we treat lungs like they’re just mechanical bellows. But they’re alive, right? Sensitive. Reactive. The scarring isn’t just tissue-it’s a story of every breath you’ve taken, every toxin you’ve inhaled, every silent cough you ignored. We fix the machine, but never ask why it broke in the first place.
Rachele Tycksen
March 26, 2026 AT 20:28so like… if i stop smoking now will it help? or is it too late??
Korn Deno
March 28, 2026 AT 01:04The real tragedy isn't the disease-it's that we wait until the damage is visible before we act. Early detection is the only real win here. And yet we still treat it like a last-resort diagnosis. We need screening like we do for colon cancer. Not after you're gasping on the couch.
Also-why is NAC still being sold as a miracle cure? It’s not. Stop wasting money.
Aaron Sims
March 29, 2026 AT 12:34Oh great, another pharmaceutical miracle! First they tell us it’s ‘idiopathic,’ then they sell us $10k/month pills that make you diarrhea-sick. And don’t get me started on ‘zampilodib’-sounds like a drug made in a lab by someone who hates humans. Who funds this? Who profits? Who gets left behind?
Meanwhile, the EPA ignores asbestos in schools, and the FDA approves drugs while ignoring environmental causes. This isn’t medicine. It’s capitalism with a stethoscope.
Agbogla Bischof
March 30, 2026 AT 22:10As a pulmonologist from Lagos, I’ve seen ILD in patients with no access to HRCT or antifibrotics. Many rely on oxygen cylinders from private vendors or homemade nebulizers. The global disparity is staggering. In the U.S., you have AI diagnostics; in Nigeria, you pray the cough doesn’t turn to blood. This isn’t just a medical issue-it’s a justice issue.
Also, sarcoidosis is underdiagnosed in African populations. The fibrosis patterns differ. Research must include global data-not just Western cohorts.
Pat Fur
March 31, 2026 AT 17:59My mom had IPF. She lived 7 years after diagnosis. Not because of drugs. Because she walked every morning. Sat in the sun. Laughed with her grandkids. The pills slowed the decline. But joy? Joy kept her breathing.
Anil Arekar
April 2, 2026 AT 10:09The scientific rigor presented in this post is commendable. The integration of clinical metrics such as FVC and DLCO with real-world outcomes underscores the necessity of a multidisciplinary approach. It is imperative that healthcare systems prioritize early diagnostic pathways, especially in underserved populations where access to pulmonologists remains limited. Furthermore, the inclusion of pulmonary rehabilitation as a cornerstone of care aligns with global best practices endorsed by the World Health Organization.
James Moreau
April 3, 2026 AT 09:56I’ve been on nintedanib for 18 months. Diarrhea’s a beast, but I can still carry my own groceries. That’s a win. I don’t need a cure-I need to keep living. Thanks for the clarity on the new drug. I’ll ask my doc about zampilodib.
Zola Parker
April 5, 2026 AT 01:12They say 'no cure' but they’re selling a $3 billion market. Coincidence? 😏
florence matthews
April 5, 2026 AT 06:07My cousin got diagnosed last year. She started rehab and now she’s gardening again. I didn’t realize how much a 6-minute walk could mean. Thanks for this. ❤️
Kenneth Jones
April 7, 2026 AT 03:07Stop giving false hope. These drugs don’t work. They just buy you a few extra months of nausea before you die. Get a transplant or don’t bother.
Mihir Patel
April 7, 2026 AT 15:59Bro I had this cough for 3 years… went to 5 doctors… they all said ‘you’re just stressed’… then one day I passed out on the subway and they finally did the CT… turns out I’m 2 years from transplant… this post is like… i wish i’d read this 2 years ago