Most people think of melanoma when they hear the words "skin cancer," but that’s actually the least common type. The vast majority of skin cancers fall under the umbrella of nonmelanoma skin cancer, which includes two primary types: basal cell carcinoma (BCC) and squamous cell carcinoma (SCC). Together, these account for about 95% of all skin cancer cases worldwide. While both are highly treatable, they behave very differently in your body. Understanding the difference isn’t just academic-it can change how quickly you seek help and what kind of treatment you need.
If you’ve noticed a spot on your skin that won’t go away, it helps to know which one you might be dealing with. Basal cell carcinoma is the most common cancer in humans, but squamous cell carcinoma is the more aggressive of the two. Let’s break down exactly what sets them apart, from where they start in your skin to how fast they grow and how doctors treat them.
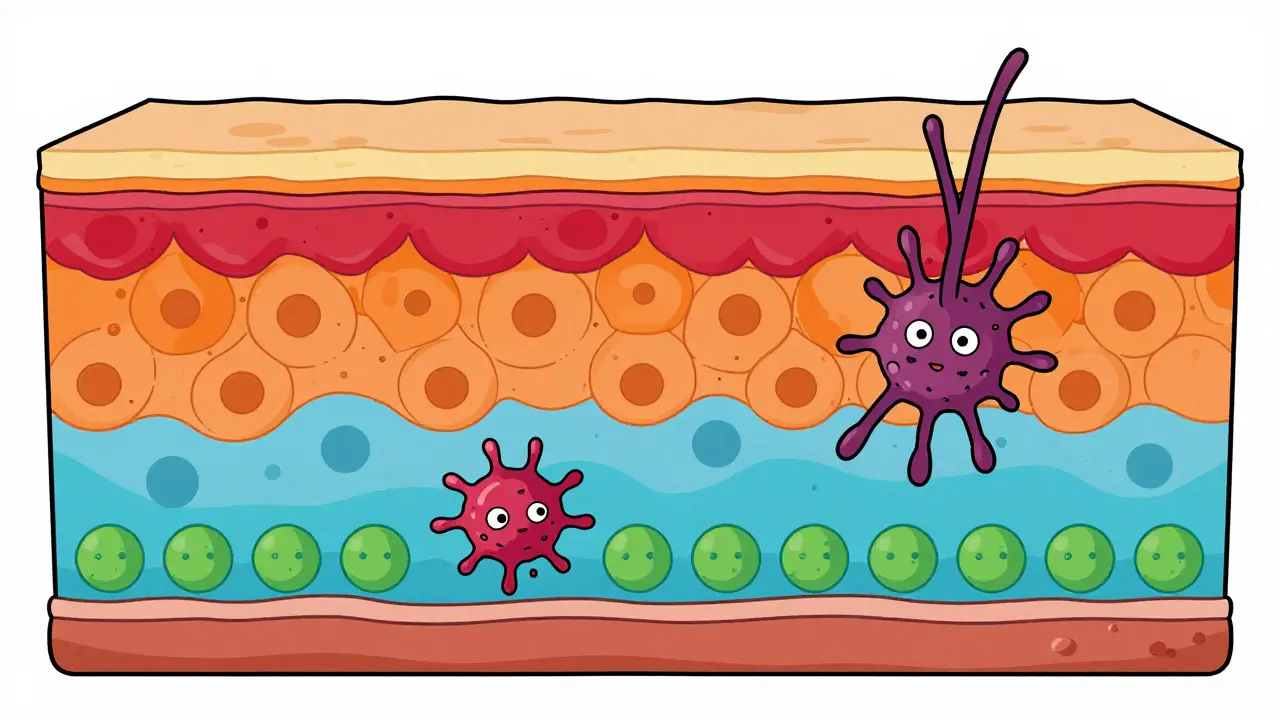
Where They Start: Anatomy of the Skin
To understand why these cancers act differently, you have to look at where they begin. Your epidermis-the outer layer of your skin-has several layers. At the bottom sits the stratum basale, home to basal cells. These cells constantly divide to create new skin cells. As those new cells move up toward the surface, they flatten out and become squamous cells.
Basal cell carcinoma (BCC) starts in that lower layer of basal cells. Because these cells are deep, BCC tends to grow slowly and stays localized. It rarely travels to other parts of the body. On the other hand, Squamous cell carcinoma (SCC) begins in the upper layers of the epidermis, among the squamous cells. This location gives SCC a slightly higher chance of spreading deeper into the tissue or, in rare cases, metastasizing to lymph nodes or other organs.
Both types are driven primarily by ultraviolet (UV) radiation exposure. About 80% of cases appear on sun-exposed areas like the face, neck, ears, and hands. However, the pattern of sun damage matters. BCC is often linked to intense, intermittent sunburns earlier in life, while SCC is strongly associated with cumulative, long-term sun exposure over decades.
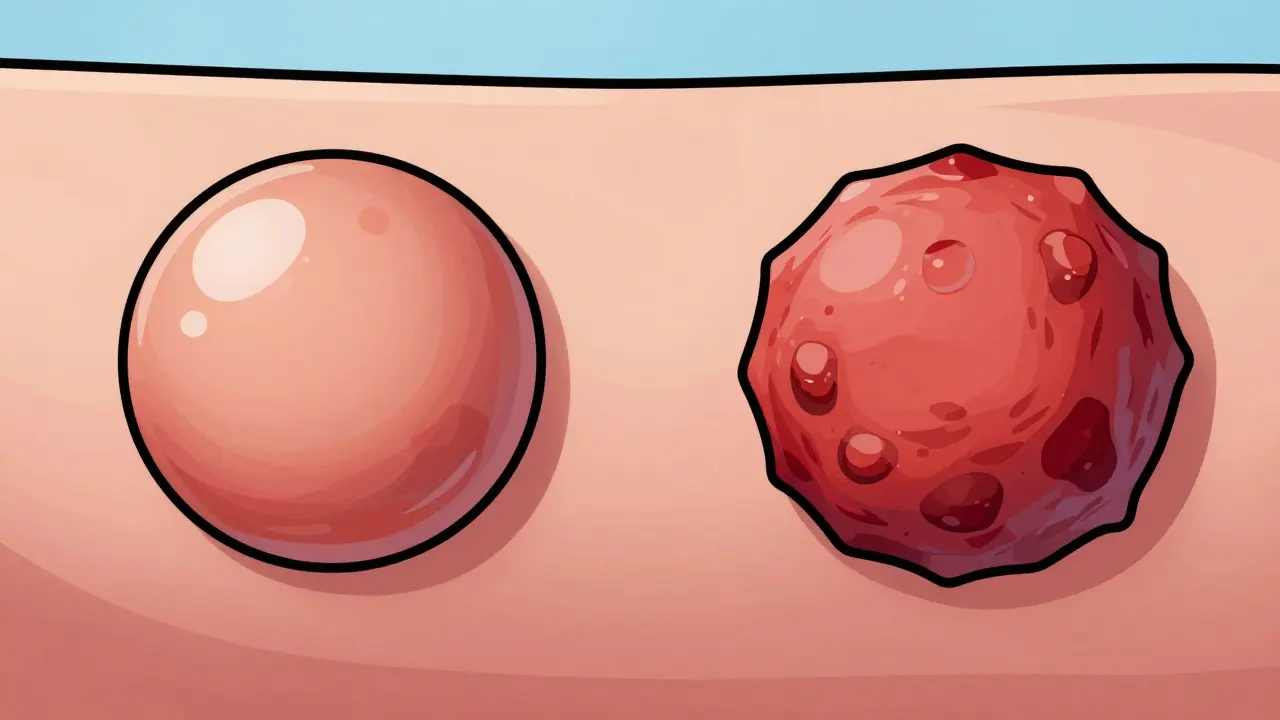
What They Look Like: Visual Signs
You can’t always tell the difference just by looking, but there are classic presentations for each. Knowing these signs helps you spot them early during self-checks.
BCC usually shows up as:
- A shiny, pearly or waxy bump (seen in about 70% of cases).
- An open sore that bleeds, scabs, and never fully heals (about 20%).
- A scar-like patch that looks white, yellow, or waxy (10%).
SCC tends to present differently:
- A firm, red nodule with a central depression (45%).
- A flat lesion with a scaly, crusted surface that may bleed easily (25%).
- A new sore or raised growth on an old scar or ulcer (20%).
- A thickened area of skin that crusts or bleeds (10%).
The key takeaway? If a spot looks like a pearl or a scar that doesn’t fade, think BCC. If it’s rough, scaly, crusty, or bleeds frequently, lean toward SCC. But remember: only a biopsy can confirm the diagnosis. Don’t wait if something looks suspicious.
Growth Speed and Metastasis Risk
This is where the stakes get serious. BCC grows slowly-typically expanding at a rate of 0.5 to 1.0 centimeter per year. It’s locally destructive, meaning it can eat away at nearby tissue if left untreated for years, but it almost never spreads elsewhere. Metastasis occurs in fewer than 0.1% of BCC cases.
SCC is faster and more dangerous. It grows at an average rate of 1.5 to 2.0 cm per year, and some aggressive subtypes can double in size within four to six weeks. More importantly, SCC has a real metastatic potential. Approximately 2% to 5% of SCC cases spread to other parts of the body. In high-risk locations like the lips or ears, that risk jumps to 9%-14%. This makes SCC the second leading cause of skin cancer-related deaths after melanoma.
Dr. John Zitelli, past president of the American College of Mohs Surgery, puts it plainly: “While basal cell carcinoma is more common, squamous cell carcinoma requires more urgent attention due to its metastatic potential.” That urgency shouldn’t be ignored.
Who Gets What? Risk Factors and Demographics
Both cancers favor fair-skinned individuals, especially those over 50. In fact, 85% of cases occur in people older than 50. The average age of diagnosis is 67 for BCC and 69 for SCC. But beyond age and skin tone, other factors play a role.
Gender differences exist. BCC affects men and women fairly equally (55% male, 45% female). SCC, however, shows a stronger male predominance (65% male, 35% female), likely reflecting historical occupational sun exposure patterns. Immunocompromised patients face dramatically higher risks. Organ transplant recipients, for example, have a 250-fold increased risk of developing SCC compared to the general population, versus only a 10-fold increase for BCC.
Geography also matters. In high-sun regions like Australia, SCC makes up 30% of skin cancers, compared to just 15% in northern Europe. This reflects SCC’s strong link to cumulative UV damage over time.

Treatment Approaches: How Doctors Handle Each Type
Because BCC is slower and less likely to spread, treatment can sometimes be less aggressive. For superficial BCC lesions, topical medications like 5-fluorouracil or imiquimod can achieve 60-70% clearance rates. Surgical excision remains the gold standard, with cure rates between 95% and 98% for primary lesions. Mohs micrographic surgery offers a 99% five-year cure rate for primary BCC.
SCC demands more robust intervention. Topical treatments are less effective, achieving only 40-50% clearance. Surgical margins need to be wider-4 to 10 mm for high-risk SCC compared to 3-5 mm for low-risk BCC. Mohs surgery still performs well, with a 97% five-year cure rate for primary SCC, but recurrence rates are higher, especially in immunocompromised patients (15% vs. 5% for BCC).
In advanced cases, systemic therapies come into play. The FDA approved cemiplimab-rwlc (Libtayo) in 2018 as the first immunotherapy for metastatic SCC, showing a 47% response rate compared to 20% with traditional chemotherapy. For advanced BCC, hedgehog pathway inhibitors like vismodegib show 85% efficacy, though no equivalent exists yet for SCC.
| Feature | Basal Cell Carcinoma (BCC) | Squamous Cell Carcinoma (SCC) |
|---|---|---|
| Prevalence | ~80% of nonmelanoma skin cancers | ~20% of nonmelanoma skin cancers |
| Growth Rate | Slow (0.5-1.0 cm/year) | Faster (1.5-2.0 cm/year) |
| Metastasis Risk | <0.1% | 2-5% (up to 15% in high-risk sites) |
| Primary Appearance | Pearly bump, non-healing sore, scar-like patch | Firm red nodule, scaly/crusted lesion |
| Topical Treatment Efficacy | 60-70% clearance | 40-50% clearance |
| Mohs Surgery Cure Rate | 99% (primary) | 97% (primary) |
Prevention and Monitoring: Staying Ahead of the Curve
Prevention works best when it’s consistent. Daily sunscreen use reduces BCC risk by 40% and SCC risk by 50%, highlighting SCC’s stronger tie to cumulative sun exposure. Wear protective clothing, seek shade during peak hours (10 AM-4 PM), and avoid tanning beds entirely.
If you’re at high risk-fair skin, history of skin cancer, organ transplant recipient-you need quarterly dermatological exams. Studies show that 73% of recurrent SCC cases are detected within 12 months of prior treatment, compared to 18 months for BCC. Regular checks aren’t optional; they’re essential.
New technology is helping too. AI-assisted dermoscopy tools now achieve 94% accuracy in differentiating BCC from SCC in preliminary trials. Photodynamic therapy improvements show 92% clearance for superficial SCC versus 85% for BCC. These advances mean earlier detection and better outcomes.
Is squamous cell carcinoma more dangerous than basal cell carcinoma?
Yes. While both are highly treatable when caught early, SCC has a significantly higher metastatic potential (2-5%) compared to BCC (<0.1%). SCC also grows faster and requires more aggressive treatment, making it clinically more significant.
Can basal cell carcinoma spread to other parts of the body?
Extremely rarely. Metastasis occurs in fewer than 0.1% of BCC cases. However, untreated BCC can cause significant local tissue destruction over time, so early removal is still critical.
What does squamous cell carcinoma look like on the skin?
SCC often appears as a firm, red nodule with a central depression, a flat scaly/crusted lesion that may bleed, or a new sore on an old scar. It tends to be rougher and more inflamed than BCC.
How quickly should I see a doctor for a suspicious skin spot?
Immediately if it’s changing rapidly, bleeding, or not healing within two weeks. Given SCC’s faster growth rate, prompt evaluation is crucial. Early detection leads to 90%+ cure rates for both types.
Are there effective treatments for advanced squamous cell carcinoma?
Yes. Immunotherapy drugs like cemiplimab (Libtayo) have shown 47% response rates in metastatic SCC cases, far surpassing older chemotherapy options. Wide surgical excision and Mohs surgery remain primary treatments for localized disease.
Why do organ transplant recipients have such high SCC risk?
Immunosuppressive medications weaken the immune system’s ability to destroy UV-damaged cells. Transplant recipients face a 250-fold increased risk of SCC compared to the general population, requiring rigorous skin surveillance.